Polycystic ovary syndrome is one of those health conditions that a lot of women have heard about, but few truly understand until they receive a diagnosis. Also known as PCOS, polycystic ovary syndrome affects how a woman’s ovaries function. It is a hormonal disorder that is surprisingly common, yet it remains underdiagnosed and often misunderstood. When we talk about polycystic ovary syndrome, we are referring to a condition where the ovaries produce an abnormal amount of androgens, which are male sex hormones that are usually present in women in only small quantities. This hormonal imbalance causes a cascade of issues, including irregular menstrual cycles, cysts on the ovaries, and difficulty getting pregnant.
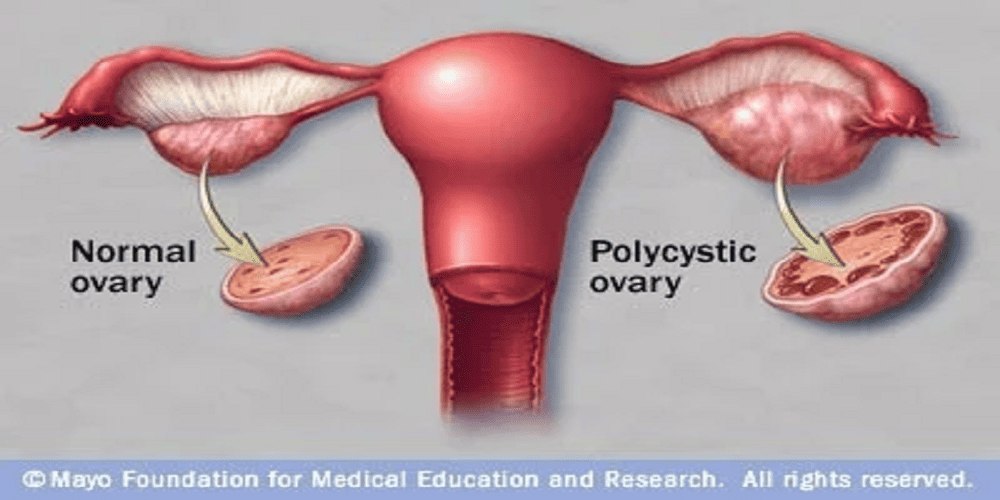
The name polycystic ovary syndrome can be a little misleading. The term “polycystic” suggests that the ovaries are filled with many cysts, but in reality, the “cysts” are actually immature follicles that have failed to release an egg. These follicles build up on the ovaries over time, giving them a string-of-pearls appearance on an ultrasound. However, not every woman with polycystic ovary syndrome will have these visible cysts, and having cysts alone does not mean you have the condition. This is a crucial distinction that many people miss. Polycystic ovary syndrome is primarily a metabolic and endocrine disorder, not just an ovarian problem.
The prevalence of polycystic ovary syndrome is staggering. Estimates suggest that between five and fifteen percent of women of reproductive age worldwide live with polycystic ovary syndrome. In the United States alone, that amounts to millions of women. Despite these numbers, many cases go undiagnosed because the symptoms can be subtle or mistakenly attributed to other causes. For a long time, doctors believed polycystic ovary syndrome was primarily a fertility issue. Today, we know it is far more complex. Polycystic ovary syndrome is linked to insulin resistance, type 2 diabetes, cardiovascular disease, and even mental health struggles like anxiety and depression.
What causes polycystic ovary syndrome in the first place? Researchers have not pinpointed a single cause. Instead, evidence points to a combination of genetic and environmental factors. If your mother or sister has polycystic ovary syndrome, your risk of developing it is significantly higher. There also appears to a link between polycystic ovary syndrome and low-grade inflammation. Many women with the condition have elevated levels of inflammatory markers like C-reactive protein. This inflammation may stimulate the ovaries to produce more androgens. Another major player is insulin. Many women with polycystic ovary syndrome have cells that do not respond properly to insulin, a condition known as insulin resistance. When the body resists insulin, the pancreas pumps out even more insulin to compensate. Excess insulin then triggers the ovaries to churn out testosterone, worsening the hormonal imbalance.
Now, how do you know if you might have polycystic ovary syndrome? The symptoms vary widely from woman to woman, which is part of what makes this condition so tricky to diagnose. Some women develop noticeable signs in their teenage years, while others do not realize anything is wrong until they struggle to conceive in their late twenties or early thirties. The most common symptoms of polycystic ovary syndrome include irregular periods. That might mean having fewer than eight or nine periods a year, or periods that come every thirty-five days or more. Some women with polycystic ovary syndrome stop menstruating entirely for months at a time. Others experience heavy bleeding when their period finally arrives because the uterine lining has had extra time to build up.
Another hallmark of polycystic ovary syndrome is excess androgen, which shows up physically as hirsutism, or unwanted hair growth on the face, chest, back, or thighs. At the same time, some women experience male-pattern baldness or thinning hair on their scalp. Severe acne that does not respond well to typical treatments is also common. Oily skin and dandruff can accompany polycystic ovary syndrome as well. Weight gain, particularly around the abdomen, is a frequent complaint. Many women with polycystic ovary syndrome find that they gain weight easily and struggle to lose it, no matter how carefully they eat or how often they exercise. Dark patches of skin on the neck, groin, or under the breasts, known as acanthosis nigricans, are another sign of insulin resistance related to polycystic ovary syndrome.
Diagnosing polycystic ovary syndrome is not as straightforward as a simple blood test. For many years, doctors relied on different criteria, which led to confusion. Today, most clinicians use the Rotterdam criteria, which require a woman to have at least two of the following three features. First, irregular or absent ovulation, which usually shows up as irregular periods. Second, clinical or biochemical signs of high androgen levels, meaning either physical symptoms like excess hair growth or elevated testosterone on a blood test. Third, polycystic ovaries visible on an ultrasound. A doctor must also rule out other conditions that can mimic polycystic ovary syndrome, such as thyroid disease, high prolactin levels, or non-classic congenital adrenal hyperplasia. This process of elimination is essential because treating polycystic ovary syndrome requires an accurate diagnosis.
Living with polycystic ovary syndrome can feel overwhelming, especially when you are first diagnosed. The condition has no cure, but that does not mean you cannot manage it effectively. In fact, many women with polycystic ovary syndrome lead perfectly normal lives, have healthy pregnancies, and keep their symptoms under excellent control. The key is a combination of lifestyle changes, medical treatments, and consistent monitoring. For overweight women with polycystic ovary syndrome, losing even five to ten percent of body weight can make a dramatic difference. Weight loss improves insulin sensitivity, lowers androgen levels, and can restore regular ovulation. This is why diet and exercise are almost always the first line of defense against polycystic ovary syndrome.
What kind of diet works best for polycystic ovary syndrome? There is no single magic diet, but most experts recommend a low-glycemic approach. That means choosing carbohydrates that do not spike your blood sugar. Think whole grains, legumes, vegetables, and fruits instead of white bread, sugary snacks, and soda. Cutting back on processed foods and added sugars can reduce insulin levels and help manage polycystic ovary syndrome symptoms. Some women benefit from reducing dairy or gluten, but that is highly individual. Regular physical activity is equally important. Exercise helps your muscles use glucose more efficiently, which lowers insulin resistance. A combination of cardio and strength training appears to work best for polycystic ovary syndrome. You do not need to run marathons. A brisk thirty-minute walk five days a week can make a real difference.
When lifestyle changes are not enough, medication can help. Birth control pills are commonly prescribed for polycystic ovary syndrome, even for women who are not sexually active or who do not need contraception. The estrogen and progestin in birth control pills lower androgen production, regulate the menstrual cycle, and reduce symptoms like acne and excess hair growth. For women trying to conceive, medications like clomiphene or letrozole can induce ovulation. Metformin, a drug typically used for type 2 diabetes, is also prescribed off-label for polycystic ovary syndrome. Metformin improves insulin sensitivity and can help with weight management and ovulation, though it does not work for everyone. Anti-androgen medications like spironolactone can reduce hair growth and acne, but they are not safe during pregnancy.
Perhaps the most underappreciated aspect of polycystic ovary syndrome is its impact on mental health. Women with polycystic ovary syndrome are three to eight times more likely to experience depression and anxiety compared to women without the condition. This is not just about the stress of dealing with a chronic illness. There is a biological component. Hormonal imbalances and chronic inflammation affect brain chemistry. The physical symptoms of polycystic ovary syndrome, such as weight gain and facial hair, can also take a toll on self-esteem and body image. Many women report feeling ashamed or less feminine because of their symptoms. Eating disorders, particularly binge eating disorder, are more common among women with polycystic ovary syndrome. If you have polycystic ovary syndrome and you are struggling emotionally, please know that you are not alone. Seeking therapy or joining a support group can be just as important as seeing an endocrinologist.
Pregnancy is another major concern for women with polycystic ovary syndrome. The hormonal imbalances that define polycystic ovary syndrome often interfere with ovulation, making it harder to conceive. However, with proper treatment, most women with polycystic ovary syndrome can get pregnant. Ovulation induction medications work well for many. For those who do not respond to oral medications, injectable gonadotropins or in vitro fertilization are options. Once pregnant, women with polycystic ovary syndrome have a higher risk of complications, including gestational diabetes, preeclampsia, and miscarriage. These risks are not a reason to avoid pregnancy, but they do mean you need careful monitoring. Maintaining a healthy weight before pregnancy and controlling blood sugar levels can significantly reduce these risks.
Long-term health risks associated with polycystic ovary syndrome are serious but manageable. Because insulin resistance is central to polycystic ovary syndrome, women with the condition have a higher lifetime risk of developing type 2 diabetes. Regular screening of blood sugar levels is recommended, especially for those with other risk factors like obesity or a family history of diabetes. Heart disease risk is also elevated in polycystic ovary syndrome. High blood pressure, high LDL cholesterol, and low HDL cholesterol are more common. This does not mean every woman with polycystic ovary syndrome will have a heart attack, but it does mean you should pay attention to heart health. Do not smoke. Keep your blood pressure in check. Get your cholesterol tested periodically. Sleep apnea is another concern, particularly for women with polycystic ovary syndrome who are overweight. Untreated sleep apnea can worsen insulin resistance and increase cardiovascular risk.
One of the most frustrating things about polycystic ovary syndrome is how differently it affects each person. Two women with identical diagnostic criteria can have completely different symptom profiles. One might struggle mostly with acne and irregular periods while maintaining a normal weight. Another might have severe hirsutism and obesity but perfectly regular cycles. This variability means that treatment for polycystic ovary syndrome must be highly individualized. What works for your best friend may not work for you. There is a lot of trial and error involved. Some women find relief with supplements like inositol, which has been shown to improve insulin sensitivity and ovulation in polycystic ovary syndrome. Others swear by vitamin D, omega-3 fatty acids, or berberine. The evidence for these supplements is mixed, but they are generally safe and may be worth trying under medical supervision.
If you suspect you have polycystic ovary syndrome, what should you do? Start by seeing a primary care doctor or a gynecologist. Be prepared to describe your menstrual history in detail. Keep a log of your periods for two or three months before your appointment if you can. Write down any other symptoms you have noticed, even if they seem unrelated. Your doctor will likely order blood tests to check your hormone levels, including testosterone, DHEA-S, and SHBG. They may also check your fasting glucose and insulin levels, as well as your lipid profile. An ultrasound of your ovaries may be recommended, though it is not always necessary for a diagnosis. Do not be discouraged if the first doctor you see dismisses your concerns. Polycystic ovary syndrome is still underrecognized, and some clinicians hold outdated views. Seek a second opinion if needed.
The landscape of polycystic ovary syndrome research is changing rapidly. In recent years, scientists have made significant strides in understanding the genetic underpinnings of the condition. Large-scale genome-wide association studies have identified multiple genetic loci linked to polycystic ovary syndrome. Some of these genes are involved in insulin signaling, while others affect gonadotropin secretion. This research could eventually lead to more targeted therapies. There is also growing interest in the role of the gut microbiome in polycystic ovary syndrome. Early studies suggest that women with polycystic ovary syndrome have distinct gut bacteria profiles compared to healthy controls. Whether altering the microbiome could treat polycystic ovary syndrome is an open question, but it is an exciting avenue of investigation.
FREQUENTLY ASKED QUESTIONS ABOUT POLYCYSTIC OVARY SYNDROME
Question one: Can you have polycystic ovary syndrome and still have regular periods?
Yes, you can. While irregular periods are a common feature of polycystic ovary syndrome, some women with the condition have cycles that appear normal on the surface. However, even with regular periods, they may still have hormonal imbalances or polycystic ovaries. This is sometimes called ovulatory polycystic ovary syndrome, though it is less common. Diagnosis in these cases usually relies on evidence of high androgens and polycystic ovarian morphology on ultrasound.
Question two: Does polycystic ovary syndrome go away after menopause?
Polycystic ovary syndrome does not simply disappear after menopause, but its symptoms often change. Androgen levels naturally decline with age, so issues like hirsutism and acne may improve. However, the metabolic risks associated with polycystic ovary syndrome, such as diabetes and heart disease, remain elevated even after a woman stops menstruating. Menopausal women with a history of polycystic ovary syndrome should continue monitoring their blood sugar, cholesterol, and blood pressure.
Question three: Is pregnancy possible with polycystic ovary syndrome without medical treatment?
For some women, yes. Many women with milder forms of polycystic ovary syndrome ovulate spontaneously at least occasionally. If you have one or two periods a year without medication, you still have a chance of conceiving on your own, though it may take longer. However, the majority of women with polycystic ovary syndrome who have infrequent or absent ovulation will need some form of treatment to get pregnant. Lifestyle changes alone restore ovulation in about fifty percent of overweight women with polycystic ovary syndrome.
Question four: Does polycystic ovary syndrome cause weight gain, or does weight gain cause polycystic ovary syndrome?
This is a chicken-and-egg question. The relationship goes both ways. The hormonal imbalances of polycystic ovary syndrome promote weight gain, especially abdominal fat. At the same time, carrying excess weight worsens insulin resistance, which in turn makes polycystic ovary syndrome symptoms more severe. It is a vicious cycle. Breaking that cycle is challenging but possible. Even modest weight loss can interrupt the feedback loop and improve symptoms dramatically.
Question five: What is the difference between polycystic ovary syndrome and simple ovarian cysts?
This is a very common point of confusion. Simple ovarian cysts are fluid-filled sacs that typically form during the normal menstrual cycle and usually resolve on their own without treatment. They are not related to hormones. Polycystic ovary syndrome, by contrast, involves many small follicles that have stopped developing and are not true cysts. More importantly, polycystic ovary syndrome is a systemic endocrine disorder affecting your entire body, while simple ovarian cysts are localized and usually harmless.
Question six: How quickly can you see symptom improvement after starting treatment for polycystic ovary syndrome?
It depends on the symptom and the treatment. Menstrual regularity often improves within one to three months of starting birth control pills or metformin. Acne may take three to six months to show noticeable improvement. Hirsutism is the slowest to respond, often requiring six to twelve months of consistent treatment before you see significant changes. Lifestyle changes take time too. Many women report feeling more energetic and having fewer sugar cravings within a few weeks of dietary changes, but weight loss and ovulation improvements usually take several months.
Question seven: Are there any natural remedies proven to help with polycystic ovary syndrome?
The term natural remedy is tricky because it is not regulated. However, some supplements have decent research behind them. Myo-inositol and D-chiro-inositol, often sold as a forty-to-one ratio supplement, have been shown in multiple studies to improve insulin sensitivity, lower testosterone, and restore ovulation in women with polycystic ovary syndrome. Spearmint tea has some evidence for reducing mild hirsutism. Chromium and berberine show promise but require more research. Always talk to your doctor before starting any supplement, as natural does not mean risk-free.
Question eight: Can teenagers be diagnosed with polycystic ovary syndrome, or do you have to wait until adulthood?
Teenagers can be diagnosed, but doctors are appropriately cautious. Many of the features of polycystic ovary syndrome, such as irregular periods and acne, are also normal during the first few years after a girl starts menstruating. Most guidelines suggest waiting at least two years after a girl’s first period before making a diagnosis, unless the symptoms are severe. In adolescents, doctors typically require both irregular periods and evidence of high androgens, since polycystic ovaries on ultrasound are common in healthy teenagers.
Question nine: Does having polycystic ovary syndrome mean you are infertile?
Absolutely not. This is one of the biggest myths surrounding the condition. Polycystic ovary syndrome is a leading cause of infertility, which means it makes it harder to get pregnant. But harder is not the same as impossible. With appropriate treatment, the vast majority of women with polycystic ovary syndrome can conceive and carry a pregnancy to term. Many women with mild polycystic ovary syndrome even conceive naturally without any medical help.
Question ten: How often should someone with polycystic ovary syndrome see a doctor?
At a minimum, an annual checkup is recommended for monitoring blood pressure, weight, and menstrual patterns. Blood sugar and cholesterol should be checked at least every one to two years, more often if you have other risk factors. If you are actively trying to conceive or having trouble managing symptoms, you may need to see your doctor every few months. Women with polycystic ovary syndrome who are on long-term medication like birth control or metformin should have a medication review at least once a year. Do not skip these appointments. Polycystic ovary syndrome is a lifelong condition, and regular monitoring is the best way to prevent complications down the road.
Leave A Comment
0 Comment